
Designing for Active Life: Moving and Being Moved Together with Dementia Patients
Helena Tobiasson *, Yngve Sundblad, Åke Walldius, and Anders Hedman
Department of Media and Interaction Design, Kungliga Tekniska Högskolan, KTH, Stockholm, Sweden
Life for older people with dementia tends to be inactive. This paper reports on two case studies in which exercise games (exergames) were introduced in dementia special care units with a focus on patients’ well-being. The first case used a participatory design (PD) approach to engage the patients as users in the process. The results highlight the patients’ enjoyment in playing these games in a socially encouraging environment. We have found that exergames in dementia care provide patients with the well-documented health benefits of physical activity and also result in social and cognitive benefits. The results indicate that the notions of games/competition, social interaction, physical activity and challenges are valuable ingredients when designing for the well-being of older people who suffer from moderate to severe dementia.
Keywords – Dementia, Exergames, Participatory Design, Physical Expression, Physical Activity, Social Interaction.
Relevance to Design Practice – Participatory design can help to reveal preconceptions and misunderstandings. Designing activities in settings such as dementia care units, where some participants suffer from an impaired ability to speak for themselves, requires a sensitive approach regarding patients’ physical expression through movement, as well as allowing time for trust to be established.
Citation: Tobiasson, H., Sundblad, Y., Walldius, Å., & Hedman, A. (2015). Designing for active life: Moving and being moved together with dementia patients. International Journal of Design, 9(3), 47-62.
Received October 2, 2014; Accepted September 19, 2015; Published December 31, 2015.
Copyright: © 2015 Tobiasson, Sundblad, Walldius, & Hedman. Copyright for this article is retained by the authors, with first publication rights granted to the International Journal of Design. All journal content, except where otherwise noted, is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 2.5 License. By virtue of their appearance in this open-access journal, articles are free to use, with proper attribution, in educational and other non-commercial settings.
*Corresponding Author:tobi@csc.kth.se.
Helena Tobiasson holds a PhD in Human Computer Interaction from KTH, School of Computer Science and Communication at the Department of Media and Interaction Design in Stockholm, Sweden. She is a European Ergonomist and a Postdoctoral researcher collaborating with the Interactive Institute and the Department of Social Medicine in Umeå, Sweden. Within the project Movement in Mind, her research focuses on methods and technologies for augmented levels of physical activity in everyday situations through a Movement Acumen Design approach.
Yngve Sundblad is professor emeritus in Computer Science and Human-Computer Interaction at KTH in Stockholm, Sweden. His research and education interests include multimodal interaction and visualisation, methods for user involvement in design, computer supported cooperation, object-oriented methods for design and development of programs and interaction.
Åke Walldius is associate professor in Human Computer Interaction at KTH, Royal Institute of Technology. He earned his PhD in Cinema Studies at Stockholm University after having worked for 20 years in video production and information visualisation. His main research interests are information visualisation, genre analysis, participatory design and quality assurance. As appointed expert in standardization (human-centred design and usability), the challenge to introduce participatory design methodology into the procurement of workplace software is a special interest. Here, he sees a great potential for information visualisation (e.g., strategy mapping) to facilitate on-going deliberations between an ever-broader spectrum of stakeholders concerned in the digitalization of working life.
Anders Hedman has a background in philosophy, computer science and psychology. His research combines these three areas. Recently, he has worked on a topic he terms ‘cognitive endurance’, a perspective on health and wellbeing that focuses on cognitive wellbeing throughout the lifespan.
Introduction
The risk of dementia increases with age. Dementia affects the reasoning abilities and short-term memory. Over time, everyday activities become difficult to manage, even with family support. Sufferers may be unable to initiate and undertake social, cultural or physical activities as they did before. As dementia progresses, it is common to move patients into special care units, since the burden on family or friends becomes too difficult to handle (Moyle, McAllister, Venturato, & Adams, 2007). In a report commissioned by the Department of Health and Aging (DoHA), the organization Alzheimer’s Australia (2011) describes how demanding dementia care is in terms of funding and the human resources needed. The report also describes a failure to meet the needs of people with dementia and their carers. It states that patients and their carers have difficulty accessing services and that the support found is often inflexible and copes poorly with their special needs. The report raises issues regarding the poor quality of care in residential facilities. It expresses the concern that 2011 reductions in funding for the dementia program risks leaving Australia unprepared for the growing numbers of individuals being diagnosed with dementia.
Researchers have drawn attention to the negative consequences of being institutionalized, such as alienation, depression and an increased sense of loneliness (Scocco, Rapattoni, & Fantoni, 2006). Caregivers need to keep in mind that these individuals have to cope with living their lives in these institutions, being permanent, not temporary, patients. There is a difficult balance in trying to provide the right amount of care while leaving some everyday tasks to be managed by the individual suffering dementia. Although there is no medical cure for dementia, physical activity is known to have positive general effects on those with dementia.
The first purpose of this paper is to report case studies on exercise games (exergames) conducted with older adults experiencing dementia. The paper discusses how exergames provide opportunities to promote self-efficacy and enhance physical literacy in older men and women with dementia. The second purpose is to share experiences of how a participatory design (PD) approach, mainly present in one of the case studies, enhanced the implementation of the exergames, resulting in their integration into the organization. We start by providing a short description of dementia, physical activity, physical literacy and self-efficacy. Next, we present exergames and describe how they have found their way into the domain of health and dementia care, often with rehabilitation as the primary focus.
Dementia and Dementia Care
Dementia is a general terminology for many diseases linked to brain-neuron death and vascular-related damage of white matter (Prince et al., 2013). Some examples are Alzheimer’s disease (AD), vascular dementia, dementia with Lewy bodies and frontotemporal dementia. AD is the most common diagnosis, with around 70% of individuals suffering from dementia having AD (Prince et al., 2013). In this setting, we use the general terms dementia or moderate to severe dementia, since these categories apply to most of our participant players.
Different methods and different scales exist for assessing levels of impairment and the progression of different types of dementia (Piguet, Hornberger, Mioshi, & Hodges, 2011). One common scale is the Clinical Dementia Rating (CDR). The CDR divides progressive dementia into five stages of impairment, where stage 4 is moderate impairment and stage 5 is severe impairment. This rating allows professionals to evaluate and assess symptoms and changes in areas such as orientation, memory, judgment, the ability to care for a household, hobbies, personal care/hygiene and community/social life.
An individual with moderate impairment needs help taking care of hygiene and assistance during chores and social activities. Disorientation in relation to time and place is present as short-termmemory is seriously impaired. The individual’s speech is also affected, making communication difficult. Individuals at this stage usually display passive behaviour and sometimes engage in repetitive activities such as wandering back and forth in corridors.
An individual with severe impairment needs support for all or almost all daily activities. Symptoms present during the moderate stage worsen in stage 5. The individual has little or no orientation in time and place. Memory loss is severe and speech and communication are difficult to initiate and sustain (Moelter et al., 2012).
Having dementia affects sufferers in multiple ways. It decreases their ability to handle everyday situations that include thinking, reasoning, communication and spatiotemporal orientation. It causes them to have increased difficulty in performing intended actions. Although basic physical ability is still present, the coordination of intentions and actions is impaired. A person suffering from dementia may seem restless and frustrated. Having dementia can also lead to aggressive and monotonous behaviour such as screaming, endless fighting and restless walking around (Van Haitsma et al., 2015). Dementia is progressive and will successively deprive an individual of control of their life. However, there are ways to positively affect the quality of life of those afflicted with dementia (Edvardsson, Winblad, & Sandman, 2008; Kada, Nygaard, Mukesh, & Geitung, 2009).
Alzheimer’s Disease International (ADI) is an international organization founded in 1984 that cooperates with the World Health Organization (WHO) on making dementia a public health priority. ADI released a policy brief in conjunction with the first G8 Dementia Summit held in London in December 2013. The report includes newly available data suggesting that the current burden and future impact of dementia has been underestimated, particularly in East Asia and Sub-Saharan African regions. The brief estimates the number of people living with dementia worldwide in 2013 to be 44.35 million; it projects this number to reach 75.62 million in 2030, before hitting 135.46 million by 2050 (Prince, Prina, & Guerchet, 2013).
Working with and giving support to people suffering from dementia is physically and mentally demanding. Relatives and staff often report a lack of ability to cope with the situation and common feelings of failure. It can be frightening not to be able to recognize the behaviour of loved ones. High levels of distress and depression have been reported among caregivers (Häggström, 2005; Coen, O’Boyle, Coakley, & Lawlor, 2002). Edberg et al. (2008) explored how nurses from three countries experienced strain in dementia care. The nurses describe their work as involving complex dealings with operational procedures, community, attitudes, other staff, patients’ family members and also their own families. Three main sources of strain were identified: being unable to “get through to them” in the sense of getting the patient to respond, recognize what is being requested of them and acknowledge the speaker when being spoken to; trying to protect patients; and having to prioritize between and balance competing needs. Research studies report misunderstandings and stigma associated with dementia. People with dementia are sometimes seen as incapable when it comes to communicating their experiences. This perception may hinder them from contributing to everyday activities for themselves and others (Jolley & Benbow, 2000; Kahana et al., 1996; Sterin, 2002). Dupuis et al. (2012) describe the exploration of a range of different methods to establish and maintain open communication with people suffering from dementia. They used both verbal and non-verbal methods, such as being attuned to facial expressions and body language:
We recognize that some partners need more time to process information and share their thoughts and value silence in our process. “Allow time for every member to share. Learn to listen and really hear what people are saying. Be careful with advice. Be generous with your questions.” (Dupuis et al., 2012, pp. 440-443)
Brooker (2007) describes person-centred care (PCC) in relation to people suffering from dementia. PCC is a set of guiding principles that supports the aim of including and focusing on the individual’s rights, values, desires and beliefs. This aim can be difficult to maintain within dementia care, but it is important to keeping patients socially active and participating in relationships with others. Brooker also describes the VIPS Framework and Tool (“VIPS” is a Swedish acronym for well-being, integrity, prevention and safety), which includes valuing people with dementia and those who care for them, treating people as individuals, looking at the world from the perspective of the person with dementia and supporting a positive social environment in which the person living with dementia can experience relative well-being. The VIPS Framework Tool was developed to provide caregivers in dementia care with a tool to assess how much their work relates to PCC. People with AD and other types of dementia are often not sufficiently well-understood and can feel alienated (Brooker, 2007).
Sjögren, Lindkvist, Sandman, Zingmark, and Edvardsson (2013) report a study on the relationship between PCC and the ability to perform the activities of daily living, quality of life, levels of pain, depressive symptoms and agitated behaviours among residents with dementia in residential care facilities. Their findings suggest a positive relationship between person-centredness, residents’ ability to perform the activities of daily living and residents’ quality of life. With the long lists of impairments due to dementia, it can be difficult to find appropriate activities for those afflicted. For example, since memory and learning abilities are affected, it can be difficult to teach new activities to people suffering from dementia.
Activity as Multidimensional
Research literature contains growing evidence that living an active lifestyle can have beneficial effects on dementia. Paillard-Borg, Fratiglioni, Winblad, and Wang (2009) state that an active lifestyle may both postpone the onset of dementia and mitigate its subsequent effects:
…our findings support the hypothesis that an active lifestyle in late life protects against dementia. A high level of engagement in physical, mental and social activities, either individually or combined, may protect against dementia; the higher the level of engagement, the stronger the protection. These findings highlight the public health importance of encouraging older persons to have an active lifestyle in order to reduce the risk or to delay the onset of dementia. (Paillard-Borg et al., 2009, p. 143)
Physical activity and exercise have many positive effects; among others, they reduce the risk of developing AD. Evidence indicates that physical activity is a preventive factor for cerebrovascular disease (Aarsland, Sardahaee, Anderssen, Ballard, & The Alzheimer’s Society Systematic Review Group, 2010). Kemoun et al. (2010) studied the effects of physical activity on walking efficiency, balance and cognitive function in patients with dementia. Their results showed that cognitive decline slowed and quality of walking improved in the tested group.
The value of being physically active does not diminish with age. For example, intensive physical training adjusted for dementia improved motor performance by engaging muscle strength and physical functioning in frail, older people suffering from dementia (Hauer et al., 2012). Stessman, Hammerman-Rozenberg, Cohen, Ein-Mor, and Jacobs (2009) report on a longitudinal cohort study where the results show that physical activity, even at a very old age, has positive effects on survival and everyday functioning. For the elderly, physical exercise and confidence in one’s ability to function autonomously in everyday life are key to supporting self-esteem and mental health (Lindwall, Rennemark, Halling, Berglund, & Hassmén, 2006). Older people suffering from dementia often find it difficult to cope with loss of function and tend to become increasingly passive (Swedish Council on Technology Assessment in Health Care, 2008).
Many studies have divided activities into mental, physical or social, examining each separately. However, activities often contain more than one of these components, Karp et al. (2006) investigating their combined effect. Their findings suggest that activities containing multiple components are more beneficial than those with one component.
Older people with dementia who live in nursing homes often lack appropriate activities. Nursing homes are expected to offer a range of activities to meet residents’ needs, but little is known about what makes activities meaningful for people with dementia. Harmer and Orrell (2008) examined what activities people with dementia living in nursing homes find meaningful. They discovered that people with dementia, their caregivers and relatives had different views. The residents found meaning in activities addressing psychological and social needs, and related to the experience of the activity. In contrast, caregivers and relatives favoured activities maintaining and training physical abilities. Although physical activity does have positive effects for dementia patients (Hauer et al., 2012; Kemoun et al., 2010), it may be difficult to motivate patients to undertake such activity.
Physical Literacy and Self-Efficacy
When undertaking physical activities, we simultaneously practice and enhance what some refer to as physical literacy, that which gives us confidence in our own physical ability and allows us to feel secure in trusting our movement abilities. Margaret Whitehead, a professor at the University of Liverpool, Department of Public Health and Policy, England, and Head of the WHO Collaborating Centre for Policy Research on the Social Determinants of Health, has initiated and promoted the concept of physical literacy as a resource for well-being across all ages. The concept is now being used and is under constant development by other researchers and practitioners in many countries. Whitehead (2010) provides a short version of the definition of physical literacy in her book Physical Literacy Throughout the Life-Course, where she remarks, “As appropriate to each individual’s endowment, physical literacy can be described as the motivation, confidence, physical competence, knowledge and understanding to maintain physical activity throughout life” (p. 11).
Another notion often described in relation to movement and physical activity is self-efficacy. It concerns the individual’s belief in their ability to perform tasks and reach goals. Albert Bandura, a professor of psychology, has been developing the notion of self-efficacy for decades and has explored it in relation to many other concepts, including promoting health through physical activity. Bandura (1994) provides the following definition:
Perceived self-efficacy is defined as people’s beliefs about their capabilities to produce designated levels of performance that exercise influence over events that affect their lives. Self-efficacy beliefs determine how people feel, think, motivate themselves and behave. Such beliefs produce these diverse effects through cognitive, motivational, affective and selection processes. (p. 71)
The notion of self-efficacy supports the understanding of different coping strategies present when handling difficult situations full of obstacles such as pain, fatigue and disability. The four following areas or factors may support the development of self-efficacy (Bandura, 1997):
- Enactive mastery experience: The person has previous experience with handling or managing the situation or task under the specific set of conditions.
- Vicarious experience or social modelling: The person sees that someone else has managed similar situations or tasks under similar conditions.
- Verbal persuasion: Positive and realistic feedback presented through a trustworthy person.
- Physiological and affective states: The person experiences the situation as positive in a psychological way. A negative experience tends to lower self-efficacy.
Exergames
During the past decade, video games have become increasingly used within fitness, health care and rehabilitation (Adamovich et al., 2005; Boulos & Yang, 2013; Li et al., 2014; Klompstra, Jaarsma, & Strömberg, 2014). The term exergame is used for computer games that incorporate physical exercise. Two commercial platforms for exergames have become popular, Nintendo Wii and Kinect. Both allow tracking and interacting with the system through body motion. Exergames seem to motivate players in ways not easily achieved through a standard repetitive and often tedious training program. Some products have been developed specifically for the elderly (Rademaker, van der Linden, & Wiersinga, 2009). Another initiative is the Rehabilitation Gaming System (RGS)—a virtual reality system. The RGS has been used in stroke rehabilitation to reduce motor deficits due to brain lesions (Cameirão, Bermúdez i Badia, Oller Duarte, & Verschure, 2010). Several research projects targeting older people and investigating areas such as fall prevention, motor learning and dementia have used parts of the standard versions of exergames (Fenney & Lee, 2010; Williams, Soiza, Jenkinson, & Stewart, 2010). In a literature review on studies making use of exergames in relation to dementia, McCallum and Boletsis (2013) present positive effects. The results are divided into categories of physical health, cognitive health, and social/emotional health.
Games for health (http://gamesforhealth.org/) is a conference series in the US and in Europe and a peer-reviewed journal focusing on exergames. During these conferences, games are discussed, from various perspectives: rehabilitation within health care, remote care settings and the use of games on mobile platforms for health.
Research Approach
We conducted the first case over five months at an elderly care unit with a special unit for dementia care and the second case over 12 months at three different elderly care units, two with special units for dementia care and one day care centre with facilities for inpatients suffering from dementia. All the care units were located in Sweden. In these case studies, we selected Nintendo Wii Sports as the exergaming platform. Our research approach is qualitative, descriptive and explorative (Holloway & Todres, 2003). In the first case, we used a PD approach. PD provides a way to reflect on prototype development in live settings, “design in doing” and observation through participation (Iivari & Lyytinen, 1998). Our generated data include interviews, citations, field notes, photographs and videos. We used a thematic analysis to discern patterns within the data. Thematic analysis consists of identifying, organizing and understanding rich collected material. It can help to interpret the research topic under investigation (Braun & Clarke, 2006). Within the research domain of human-computer interaction, thematic analysis has been used and described as valuable for evaluation and informing design (Pykhtina et al., 2012; Toth et al., 2012).
In Scandinavia, PD research projects focusing on user participation, cooperation and design have a long tradition, dating back to the 1970s (Bødker, Ehn, Sjögren, & Sundblad, 2000). Ehn (1992) described the tool perspective of early PD in which technological solutions were seen as an extension of known work tools. This perspective encourages the designer to understand the specific labour process of using work tools. As described by Ehn (2008):
Participatory design started from the simple standpoint that those affected by a design should have a say in the design process. This was a political conviction not expecting consensus, but also controversies and conflicts around an emerging design object. Hence, participatory design sided with resource weak stakeholders (e.g., local trade unions), and developed project strategies for their effective and legitimate participation. (p. 94)
Several researchers have articulated the value of participation in design methods and processes (Bannon & Ehn, 2012; Bødker & Sundblad, 2008; Seravalli, 2013). PD has been used in many research projects within the arena of human-computer interaction, from democracy at the workplace to health care, public spaces and marginalized social movements, and for democratizing innovation (Björgvinsson, Ehn, & Hillgren, 2010, 2012). In PD, skills and knowledge are collected, communicated and transformed through collaborative making. The making is often performed during workshops, where participants articulate their ideas and desires through discussion and prototype production. Different takes on PD have been used when approaching the domain of dementia care. Hendricks, Truyen and Duval (2013) provided guidelines for setting up PD projects with people suffering from dementia. They conclude that the guidelines are preliminary and note that it is challenging to collaboratively design with people who have dementia. Robinson, Brittain, Lindsay, Jackson and Olivier (2009) used PD in workshops where they developed prototypes together with people who had mild to moderate dementia and who, although still living independently, were concerned about wandering and its augmented risk of getting lost.
Our rationale for applying PD in the first case study was to get everyone involved, that is, people suffering from dementia, their relatives and caregivers, managers at the care unit and enrolled nurses to enhance active participation and collaboration. Our hope was that the PD approach would support the transformation of the exergame activity, making it “theirs” and making participants want to continue playing after the project ended.
Throughout the two cases, we used participative observations and field notes to collect data (Emerson, Fretz, & Shaw, 2001). Participative observations are helpful in obtaining information about a setting, including both the human aspect and the social environment. Some players in these cases had impaired language abilities due to dementia, making participative observation especially helpful and important. We observed body posture, the ability to perform the physical movements needed for gaming, range of motion and flow in movement. In addition, we observed how the gamers positioned themselves in the room, how they interacted with fellow gamers, caregivers and relatives and their bodily and facial expressions of failure, success, boredom, concentration or competition. We received many reflections from the caregivers’ observations directly at the setting, as well as through phone calls and emails.
Recording the participants’ actions through video allowed us one more method to collaboratively discuss, analyse and evaluate the gaming situation. Although we had not considered this aspect, our gamers requested to see the video of themselves playing, so we showed it to them. For the first case study, we recorded a total of ten hours of game activity and interviews. For the second case study, our aim for the video recording was twofold. Firstly, we aimed to continue to collect data on physical interaction in the game situation. Secondly, we aimed to produce an inspirational and instructional video that would include play, environmental information and interviews to be distributed among actors in the elderly care domain.
Altogether, we collected nine semi-structured and video-recorded interviews with participants such as managers, nurses, gamers, rehabilitation assistants and physiotherapists. We observed and collected data while playing the games ourselves along with different participants or as active spectators. Workshops were conducted for redesigning the gaming console and developing a manual for managing the game system. We also collected data in other contexts, such as during coffee breaks, while chatting, during phone calls and through emails.
Method
The first case study took place at the dementia care unit in an elderly care centre in Ockelbo, Sweden, hereafter referred to as dementia care unit A. We spent one month of preparation to purchase, arrange and set up the exergame system. Next, participants played the games over a period of four months at three hours per interval, two times a week. The whole organization was included in the aim of motivating older people with dementia to learn, manage and enjoy exergames. This inclusion involved using the PD approach. The second case study occurred at three different elderly and dementia care centres located in Umeå, Tierp, and Ockelbo, Sweden, hereafter referred to as units B, C and D. All sites are geographically situated in the northern part of Sweden. The municipality managed special care units A, C and D. B was under private management.
We ran the second case study over a period of 12 months. During this time, participants played exergames one to two times a week for about three hours each time. The timeline for the two studies was chosen to have the opportunity to establish trust and relationships with the different sites and in the different contexts. Eight months passed between the two case studies due to a delay in funding. As we started on our second case study, we learned that some of the first case study’s participants were still playing at Ockelbo and that others had joined in at unit D—a newly built elderly care unit. This was an encouraging result for the PD approach we applied in the first case study.
We looked among the residents and their caregivers and relatives for individuals who were willing to participate. In the first case study, 10 participants signed a written confidentiality agreement stating that they consented to the data collected being analysed and made public. In the second case study, we contacted or were contacted by caregivers from the three sites ultimately selected. The confidentiality agreement in the second case study was an oral approval. After consulting with their organization and with each other, 12 gamers and their caregivers and management gave their oral approval to be documented and to have the material shared with a wider audience. Thus, we had a total of 22 participants with ages ranging from the late 70s to the early 90s; 14 were women and 8 were men. Table 1 provides an overview of the structure of the two cases. All participants were diagnosed with dementia in moderate to severe stages. Some were in wheelchairs, others used walking frames and some could walk on their own. Some had physical impairments due to stroke, such as limited motor function on one side of the body. Additional gamers participated later in the study, but we focused primarily on the first 22 who had signed up at the start. From a PD perspective, the target group of stakeholders included gamers, their relatives and friends, caregivers and other staff such as janitors, administrators and managers.
Table 1. Representation of the structure of the two case studies.
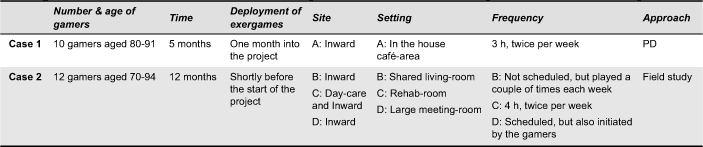
In the beginning of the first case study, we arranged design meetings with the caregivers to let them familiarize themselves with the games. We also arranged design meetings with the users and their relatives to get them interested in participating and to help them decide whether they wanted to be part of the study or just to play.
Game Context in the Different Settings
At site A (case 1), the exergames were placed outside the locked dementia ward in an area where residents often passed by and thus could easily decide to participate. The organization held other events in this area, such as Friday café, bingo, sitting gymnastics and singing. The area was open and easy to reconfigure according to the number of attendees. Instead of a TV set, we used a projector, motivated by an idea of “the bigger the better” immersion for both gamers and spectators. A workshop with the caregivers was held, during which a manual for the system was produced. We agreed on text and pictures to make it obvious what steps to take to handle the system. Starting the system was too tricky for the gamers and they got annoyed if we as supporters took too much time to get it running.
At site B (case 2), a flat-screen TV was used, and was placed in a living room with sofas, tables and chairs. The room was designed for watching TV and the setting made it inviting to sit down and be a spectator. The room was reconfigured when exergames were played. At such times, tables were moved to the sides and chairs without armrests, allowing for greater freedom of movement, were added.
Site C (case 2) has a facility for the short-term support of older patients, including a service with a focus on physical training. Outpatients as well as those in residence were welcome to participate. Here, the exergame system was placed in the same room as other training gear, such as balls, benches and so on. The video was projected onto a screen that was put up for each occasion. The exergames were seen as rehabilitation training in the spirit of competition and sport. Two rehabilitation assistants, an occupational therapist and a physiotherapist, ran the rehab. Older outpatients, as well as the individuals suffering from dementia and other inpatients at site C, could play twice a week, once for half a day and once for a full day.
Site D (case 2) in Ockelbo is a modern, newly constructed home for seniors. At the time of the second case study, the interior was not completely finished. The Wii-based exergaming system was housed in a cabinet on wheels and had to be set up for each gaming occasion. This was a hazard in comparison to the first installation at site A, where the system was set up and ready, making it easy to start playing. The system in site D will be permanently installed in a room along with other equipment for play and physical activity at some point in the future. Since many things were not in order, participants did not get to play as often as they would have liked to. The caregivers told us that residents asked about the game and when there would be more opportunities to play.
Case 1: Ready, Set, Game
In the first case study, the game was up and running. We explored alternative ways to interact with the system that might allow those with impaired physical ability to make the proper movements and to have an approximately equal chance as those without impairment when performing actions such as a full golf swing. Our method of instruction was often physical. We used touch and supported participants’ movements with our hands and with our arms placed over their hands and arms in order to guide their movements (see Figure 1). Much to our surprise, we soon realized that they wanted to compete. We had explained to the gamers that the gaming exercise was not about competing, but about having fun together. The caregivers briefed the gamers in the same way, yet they too got the impression that for the gamers, the competition was important. As a consequence, we put up a board with match results, personal records and photographs.

Figure 1. Initial physical support during the first and second case study.
The gamers became increasingly secure with the situation. Although due to memory difficulties, they told us “I’ve never done this before”, it was obvious from how they handled the console and system that on some level, they did remember their movements. They also started to both support and hassle each other competitively through speech and body language. Figure 2 shows some of the reactions to the gameplay.

Figure 2. Concentration and happy failure.
Although initially reluctant to play, many of the caregivers shared their experiences of playing with the gamers as being more positive than they could have imagined. During our design meetings, it became obvious that gaming needed to be incorporated into the caregivers’ assigned work for them to feel that they had time for it. As researchers, we managed to bring this information to the managers, who were positive towards the activity and who made it part of the caregivers’ job description. Stories started to spread about who managed to score and who played with whom.
One story is about a relative who got a phone call from one of the gamers in which the gamer excitedly said, “I won, I won!”, but was unable to explain what had been won. The relative called the special housing facility to find out.
Caregivers and other staff also used the Wii system among themselves. Another story is about a caregiver who forgot that she had finished for the day because she was “immersed in the match”.
Together with the caregivers, we found new words to instruct and support the gamers in their interaction with the system. Judging only from the words, it would probably be difficult to understand that we were instructing them in golf, bowling, boxing or fishing. The gamers learned new expressions, although they sometimes mixed them up, such as when announcing “I got a stroke” instead of “a strike”. We were surprised at the level of detail the gamers noticed on the screen. They commented on the bird song, the green grass and the trees on the golf course.
Initially, we were worried about how we would manage to explain the functionality of the system or respond to the gamers’ technical questions. We were surprised and relieved that they seemed not to bother with or question the fact that they can “bowl” in a corner of their dementia care unit. As time passed, we saw more and more initiative from caregivers and gamers to “go for a match”.
After some time, we found that around an hour of active play was sufficient, even if the gamers sometimes played for up to two hours. After a while, the gamers become more secure in their movements and in how they positioned themselves in front of the screen. Some wanted to let go of their walker while swinging in golf or while bowling. They put increasingly more force (see Figure 3) behind their movements. It became evident from the colour in their faces and the sound of their breathing that they were having a workout. Some said they got sore muscles. We looked for other games than those involving competitive sports and found ice-skating, snowboarding and fishing. During the second project and with the return to Ockelbo, we were happy to discover that the original participants were still playing. Many more wards had also bought exergames systems.

Figure 3. Forceful actions in order to score.
Case 2: The Three Sites—Up and Running
In the second case study, the three sites had already started to use the exergames. They had applied different focuses, some on rehabilitation and others on social aspects. The sites approached us because they knew about our first case study and wanted some support. This suited us well, since we wanted more opportunities to collect data. One of the three sites was the original site in Ockelbo that had now moved to a newly built elderly care unit with several departments for dementia care. On their own, they had continued to apply a PD-oriented approach and had included as many people in the organization as possible in their exergame development process. At the other two settings, the exergames were in the hands of the rehabilitation personnel. We spent about one day a week at each of the three sites in our follow-up study.
At site B, some of the residents suffered from post-stroke disabilities causing weakness and loss of motor function. Through the Wii system, they had a new opportunity to practice their balance, motor skills and concentration, while being occupied with scoring in bowling or winning a race in kayaking (see Figure 4 for gamers in action). These activities were very different from traditional rehabilitation.

Figure 4. Participants with different physical abilities were still able to score.
A rehabilitation assistant shared that she had observed many situations of fun and laughter during the Wii training sessions. She noted that it seemed easier for the gamers to perform numerous repetitions of a movement while immersed in a game or sport situation. We asked the gamers what type of activities they used to do earlier in their lives. Some of the men said that hunting had been a central activity, so we found hunting games and tried them with the gamers. The hunting games came with a rifle attached to the console (see Figure 5). Animals appeared at a distance and it was difficult for the gamers to get closer. The only animal the gamers managed to hunt down was the hunting dog. This produced plenty of laughter, but no success in scoring.

Figure 5. Hunting animals out of reach.
At site B, the situation was focused on using the system as entertainment. The gamers played when we were present or when the physiotherapist had the time. It was not a scheduled activity or something that was open for other categories of caregivers to use. The physiotherapist would bring the game system in a box and set it up, using the TV as monitor. Gamers seemed to enjoy the table tennis, although sometimes they needed initial support to get the interaction right. Wakeboarding (see Figure 6) and biking were also popular.

Figure 6. Enjoying virtual water activities.
Other games like archery were available, but included too many steps for these gamers to master. Not everyone was eager to play, although there was a group of five or six gamers who actively played. About the same number of patients were spectators. They started commenting on the game, as some of the situations reminded them of things they had done in their earlier days. In wakeboarding, gamers performed a great range of movements, crossing the vertical midline and sometimes reaching over shoulder level. As an example of how they seemed immersed and engaged in the exergames activities, gamers often made sounds to underline the wakeboard hitting the surface after a jump or supported themselves by cheering.
During case 2 at site D, the structure from case 1 site A had been kept, in which the caregivers could list gaming as a work task. Gaming was scheduled, but could also take place at the initiative of the gamers. Some of the gamers were now “experts”, as they had been playing since the start of the first project. Others were beginners. This gave the expert gamers the additional role of being instructors.
Redesigning the Console
For some of the gamers, the handling of the console was problematic due to dry hands. The console slipped, turned and twisted in their hands. Furthermore, due to muscle weakness, deficits in the coordination of small movements and motor deficits, some of the elderly gamers pressed too many buttons at the same time, causing interruptions and often ending the game unintentionally. The gamers commented on the slippery surface of the console and on other design issues of the console, such as it being easy to press too many buttons at the same time.
In light of these issues, we arranged design workshops to try to find a solution, focusing on the design of the console. Console prototypes were collaboratively developed and tested during two design workshops. In addition to the gamers, an occupational therapist and an enrolled nurse participated in the workshops. Different materials were tested, paper, plastic and a thermoplastic splint. The thermoplastic splint was used in the final prototype, as it was easily moulded by heat. The two workshops resulted in an alternative console design with a lid (see Figure 7). It was designed to be easy to grip and to keep gamers from pushing buttons inadvertently. The redesign workshop was done during both case 1 and case 2. The gamers in both locations preferred the adjusted console because it was easier to hold and it kept them from accidentally restarting the system.

Figure 7. Working the adjustment material and the final lid.
Analysis and Results
The material on which we base our analysis derives from field situations (Rogers, Sharp, Preece, & Tepper, 2007) and consists of verbal expressions from and observations of gamers, caregivers, relatives and managers. We collected this material during interviews, workshops and game-playing. Sounds of heavy breathing due to the physical movements performed while playing or emotional and social expressions such as glances, smiles and facial expressions of failure may have been lost along the way from the actual event to the translated text. Therefore, we have tried to describe the situations with as much detail as possible in order to transmit the actual experience. In a design-oriented manner described by Bamberger and Schön (1983) as “conversational learning”, we have “listened” to the material during the thematic analysis and let the material speak back to us.
We carried out the thematic analysis based on empirical data that was generated through different methods. After transcribing the recorded interviews into texts and gathering other types of generated data such as field notes and photographs, we approached the rich material through reading, discussing and reflecting to identify patterns by clustering similarities in the material. The next step was to organize the material around themes by which the clusters could be headed. In this way, we developed an understanding of the material. The use of photographs and video helped to underline the text and was of great support when trying to understand the rich material. The themes or categories that evolved were: the challenge of learning, the action and experience of physical movement and social interaction. We then discussed these themes in relation to theories and notions such as physical literacy and self-efficacy to further enhance our understanding.
The Challenge of Learning
This category was based on comments and observations that depict the challenge of learning how to handle the console and the challenge of learning the game structure (the output on the screen). The gamers asked about where to press and when. They struggled with coordination between their perception of what was happening on the screen and their actions. They also grappled with setting up the system. The fine motor skills that they needed to play seemed tricky for some of the gamers:
It really depends how you hold that thing. (Gamer 1)
The handling of the console seems to be tricky—to press and let go at the right moment and not press any other button. (Observation from researcher)
Some gamers showed frustration and some lost interest or commented on their own performance in a negative way. On the whole, however, the gamers found the challenge of mastering the console stimulating. They learned something new and managed to handle a device that was not primarily designed “for the “old” and “crippled”, as one gamer commented. Once they had successfully learned to handle the system, their physical ability was sufficient for mastering the console well enough. This mastery of the console relates to the theory of physical literacy, since mastering the game system provides a gamer with the experience of a body and physical abilities that still function. In other words, gamers find that can still trust and rely on themselves, giving them confidence in these activities, that their physical ability was not failing.
Some gamers had difficulty figuring out where they were on the screen. They sometimes experienced the graphics as messy and confusing. Knowing directions and where to aim in games like golf sometimes proved difficult for many of them. In taking turns, the gamers often lost track of their own whereabouts.
He jumped over again—he’s jumping over now too—this was miserably bad. (Gamer 9)
Where should I head for now then? (Gamer 14)
Can you see that little map?—It gives you an image of where you are at the moment (Researcher)
Where’d he go? There’s a hole over there as well. (Gamer 5)
No, that’s you (Researcher).
Have I turned red? (Gamer 5)
Then again, the caregivers shared a story about how some of the gamers managed perfectly while playing all by themselves and enjoyed their experience. As a caregiver or any other category of personnel, it takes a certain amount of flexibility and creativity to instruct and explain in simple words what to do and what actions to perform.
The participants seemed to be motivated by the psychology of gaming, that is, something was at stake for them in the game. They could win or lose and they could learn to master the game by playing it. Outside of the gaming events, their days were filled with the same activities and variation was scarce. In addition, any variation in activities often declined over time due to the participants’ gradual loss of motor and cognition abilities.
Observations of the way the gamers handled the actions in the different games revealed contradictions in how they talked about their gaming performance and how they actually performed. They often said that they had never tried a game before, despite having done so, and stated that they did not know how it worked or what to do. But from what we could observe, the gamers knew more than they thought they did. They had acquired procedural memory, although they contradicted this memory verbally. There was no trace of declarative memory, but their bodies knew what to do. They demonstrated a physical skill.
I’ve forgotten how to do this. (Gamer 4)
I’ve never done this and I don’t remember. (Gamer 11)
When changing games, they need some support. (Researcher field notes)
To be motivated and feel that something is at stake, a gamer needs to physically and cognitively learn how the games are played. The staff noted that this was indeed happening and in a positive way.
The thing I like the most is to see how they wake up by learning something new. With them, it’s mostly a case of preserving skills like getting dressed and managing the situation with eating. (Enrolled nurse)
The gamers also helped to create a communal spirit that promoted learning. They commented on their own and each other’s play in fun-loving ways.
Last time I played I got three strikes in a row. (Gamer 1)
You’ve played more often than me—look how good she is. (Gamer 8)
Opportunities to learn new things in a highly engaged and social manner are not normally common in the care of older people.
The first category, the challenge of learning, relates to two of the four motivating factors in the notion of self-efficacy; the enactive mastery experience (the most influential source) and the vicarious experience (Bandura, 1997). The gamers had their self-efficacy boosted by managing to master and score in the exergames. They reflected a feeling of having the skill to control the situation and finding it worthwhile to learn to master the game when after a number of game sessions they experienced competence and skill, despite some of them tending to cognitively forget their accomplishments. In addition, the vicarious experience of watching fellow gamers mastering the exergames seemed to enhance individuals’ learning as well.
The Action and Experience of Physical Movement
This category includes comments and observations regarding how the gamers made physical movements and how we as designers and caregivers instructed the gamers to perform these movements. The gamers felt good about having engaged in physical activity. Even though some reported that their arm hurt or that they became tired, they commented on the activity as something they enjoyed. They enjoyed using their bodies and appreciated sitting and relaxing after the physical activity.
My arm gets tired after playing for some time. (Gamer 17)
It’s a good feeling to feel that you’ve used your body/done something physical. (Gamer 2)
There’s also some physical training in that. (Gamer 11)
It’s good to work with the body. (Gamer 16)
The exergames provided the opportunity to experience the difference between physical activity/load and rest and allowed gamers to experience their physical ability as functional, that they had what it took to play. They were in control.
Is it better to stand? (Caregiver)
Yes. This is good for me. (Gamer 9)
They didn’t say “Oh no, now I’ll sit”, they were all red in the face. Their movement improves if they stand—they can feel it, you can see and tell that they’re excited: “Is it my turn now?” The game invites them to move. They automatically get the physical movement. (Enrolled nurse during interview)
A competitive spirit was also present during gaming. The gamers moved to score, to win, to master and to have fun and also for the sake of the movement itself. As a result, they trained their balance and the physical activity increased their blood circulation. Their bodies received healthy stress during gameplay. All this happened while they were absorbed in gaming.
Now I’ll put all the force I have on this. (Gamer 7)
Don’t use so much force now. (Enrolled nurse)
He jumped over. (Gamer 7)
The movement has gotten much smoother. Not so much fiddling and fewer questions—more game. There are bigger movements and more power behind the strike. (Researchers’ observations)
The gamers experienced mastering something, a situation that was opposite to their more typical experience of losing functions and skills. They also received extrinsic motivation to adjust and modify their movement scheme, something that is not obvious in the traditional physical training provided at the care units. The gamers did something that urged them to concentrate on what was happening on the screen, outside of their own bodies, yet they were also motivated to move. They had the opportunity to perform a variety of physical movements in different games. They seemed to like using maximal force, even though they knew this was not what the game required.
The results in this second category are related to the positive effects of physical activity. Even though heart rate or energy expenditure were not measured, changes in breathing patterns, skin-colour and how the gamers stretched and used considerable physical force were observed. The gamers also explicitly expressed their experience of having been physically active—the good feeling they got from such activity. The fourth motivating factor in the notion of self-efficacy, physiological and affective states, (Bandura, 1997), seemed to be present as well, in the gamers’ comments about how the physical activity in the exergames provided physiological and affective states such as having tired arms, heavy breathing and the feeling of a body that had been in use. The sensations of mastering, winning, scoring and “sweeping the floor” in a competition enhanced the participants’ physical literacy (Whitehead, 2010).
Social Interaction
In this category, the comments and observations concern success and failure during play: cheering, teasing, coaching and competing, the social interaction between gamers, their caregivers and others participating in the game. A conversation arena was created through the exergames, giving the gamers something in common that they could discuss and comment on.
Well, you’ve done really great. (Gamer 10)
Why did they not fall down? (Gamer 13)
Yes, they’re frightfully stubborn. (Gamer 10)
Designing or creating an arena for collaboration or social interaction among older people on a ward for dementia patients can be difficult. The game situation interests and motivates the gamers to discover and socialize with their teammates or competitors.
After moving down here—one usually isn’t busy with so much to do. (Gamer 5 during interview)
It’s more fun if there are some more exciting things. It keeps the brain alert to compete—it gets too boring otherwise. (Gamer 1 during interview)
He wanted to sit around and watch but didn’t want to play, but really was eager to watch. (Enrolled nurse)
There were many comments on the difficult balance of finding activities that motivated the residents to participate. At many care centres for older people, the activities are somewhat tranquil. With the exergames, something was happening there and then and the outcome was unclear. Something was at stake—the participants could win or lose. This situation was in stark contrast to the usual routine at these care centres, where days can be filled with the same routine without much variation, challenge, excitement or muscle tension.
Are you eager about the ranking? (Gamer 17)
The gamers frequently teased each other and commented on each other’s instinct to win. The experience of being better than someone else appeared to add to the motivation to perform. This provided an arena for fun and positive feelings.
You feel like you’re somewhat better than someone else—I felt I was competent in a way. (Gamer 1)
It’s been good to see them, watch them—you could tell they had fun. (Comment from caregiver)
They become more alert after playing and seem to carry a good feeling for quite some time after. (Comment from caregiver)
I didn’t expect it to be such a success. (Manager)
For our users with dementia who often get stressed and worried during other activities, we see that they can concentrate for a longer period of time than they usually can. (Comment from caregiver)
Gaming introduced new opportunities to socialize as the gamers discussed their status in the game, the questions of who was about to win and who was about to lose were given equal attention. The game situation created an arena for engagement that included spectator involvement as well. The spectators cheered and jovially teased the gamers. Their enjoyment was visible in how their eyes lit up and in the postures of their bodies. The cheers from the audience, who smiled, raised their hands and commented on the achievements of others energized the gamers. The gamers clearly enjoyed being perceived as something more than patients. Social interaction, the third category, can be linked to verbal persuasion, the second motivating factor in promoting self-efficacy (Bandura, 1997). Verbal persuasion from project leaders, fellow gamers, the audience, caregivers and other staff telling the gamers they were doing well seemed to influence their perceived capabilities and their motivation to be active in the game. It is worth mentioning that both the teasing and the cheering seemed to have equal impact.
Exploring Participatory Design
The second aim of this research was to explore what PD as an approach could bring to the dementia care domain. In the first case study, PD was used throughout the whole project. In the second case study, we “entered the scene” after the exergames had already been introduced by the physiotherapist and the occupational therapist in two of the three places. On the organizational level, PD provided an arena for discussion and reflection as well as a starting point for a change of perspective. By including different professionals and the gamers in the design of the intervention, the exergames activity became integrated with the organization and familiar to everyone working at the special care unit. In the two cases where the exergames were in the hands of the physiotherapists and occupational therapists, they were perceived as activities brought to the centres by experts. We saw a strong statement of the positive value of PD in special care settings on our return to Ockelbo after eight months for the second case study when we found that the patients were still playing. On the individual level, PD enhanced our aim to approach dementia patients from a resourceful and inclusive perspective.
Discussion
We set out to explore whether exergames would appeal to people suffering from moderate to severe dementia. Exergaming had several benefits that fell under the three thematic categories that we described earlier: the challenge of learning, the action and experience of physical movement and social interaction. These categories presented opportunities to promote self-efficacy and enhance physical literacy for the participants. We will now discuss these categories further.
The challenge of learning: It was not only the gamers who had to face the challenge of learning. It was also a challenge for us, as researchers, not to give in. The success was not at all immediate, we had to endure a considerable period of ambiguity, frustration and embarrassment (i.e., how could we even think that this would work?). In this category, we can also include the way the organizations managed to change and find a new way to expand their activity repertoires. In addition, we as researchers and the workers at the care units had to confront our own preconceptions and biases about what dementia patients could manage and enjoy. As Brooker (2007) also found, our research in the use of PD in the first case demonstrated how dementia is surrounded by misunderstandings.
The action and experience of physical movement: The gamers’ motor behaviour changed during gameplay. For example, some of those in need of a walker often left their walker behind in order to have a better chance of scoring. As the gamers aimed at scoring, they forced their bodies to perform and stretch far beyond what was observed in their standard daily activities. This activity provided them with an occasion to train their balance in a joyful way. The gamers described the good feeling and joy of having used their bodies. The games helped to give purpose to movement. For example, the ability to extend one’s arm to full length is not particularly meaningful if there is little opportunity to use such motion in everyday life, so its utility within gameplay gave this movement significance. In the everyday routine of the special care units, the patients had no dedicated task other than caring for themselves. The exergames provided opportunities for the dementia patients to experience their ability to still master activities, still be in the game, still manage to have control, to score and to socialize. In other words, the exergaming activity managed to promote self-efficacy and enhance physical literacy. This activity may also be described as a way of promoting health and well-being for this group of patients who know there is no cure for their situation. One could argue that any intention or attempt to bring new activities into these domains has the potential for similar positive results. Although this might be true, one can however assert that the exergame activities allow participants with different disabilities to play in a given situation, providing an arena for a “fair match”. The digital situation lacks many of the perspectives that are present when, for example, one is outside performing a water sport such as wakeboarding, getting wet from real water and smelling the salt of the sea. However, the positive feelings that are prompted by the digital situation are real and bring some of the flavour of that activity directly into a person’s everyday life at a special care unit.
Social interaction: This is an important part of the results and was a major achievement in these two case studies where the game-settings inspired our gamers to socialize. The patients were provided with something to reflect on, away from the decline of their mental and physical states. Of course, other items of positive value for the care of dementia patients were present at the care units. However, the mix of physical, cognitive, and social challenges in the exergames used in these two case studies is quite rare. As described by Harmer and Orrell (2008), dementia patients find meaning in activities that address their social needs. By providing opportunities for social interaction in these case studies, the patients’ social skills were “exercised”. This result is of great importance as social interaction skills prematurely deteriorate from lack of use. We ourselves experienced despair when observing the scarcity of these patients’ opportunities for social interaction, how few their visits with friends and family were and how lacking in variety their everyday lives were within the settings to which we had been invited.
We argue that these two cases are examples of a change from matters that focus mainly on care to matters of active participation, from monotony to autonomy and from being cared for to being in charge. To live facing life head-on is a challenge with dementia. Providing patients with a broader repertoire of things to talk about and giving them the opportunity to be viewed as gamers and not only as patients, connects to the healthy parts that are still present in these frail older people. The gamers/patients in these two case studies experienced the feeling of still belonging to the active world and of participating in activities that other people, all people, anyone, may do. Rather than receiving the impression that everything had to be adjusted for them, they realized that they were still able to master, score in and succeed at an activity that also provided content for stories that could be told and shared.
The participating gamers cooperated in redesigning the gameplay. They developed both a body language and a verbal language for the activities that were somewhat different from what are commonly seen in exergames. They also participated and cooperated in the redesign of the console.
We will now discuss the relation between the PD approach and the qualitative findings. The PD approach proved to be a powerful tool when introducing and implementing challenging activities within a user group that is often regarded as one that passively receives care. In addition, using the PD approach exposed preconceptions and prejudices from researchers, caregivers and managers. The participants possessed much more physical power and showed much more active engagement from various perspectives, as well as endurance in the exergame activities than was anticipated. PD, which was mainly used in the first case study, seemed to play an important role in helping to unveil and discover these alternative perspectives on participation. PD introduced opportunities for reflection and thereby seemed to have the potential to support change, both on an organizational and on an individual level. Through the use of PD, it was possible to discover that a change in work routines was needed for the exergame activities to become a part of the job for different types of caregivers. This organizational change was not the direct focus, rather, it came as an added value through the PD approach. In summary, through our use of the PD approach the following categories evolved:
- Competition: Instead of trying out the different games from a movement perspective, as initially proposed by the researchers, participants engaged in competition.
- Inclusion in the daily routines or agendas for the caregivers: Rather than being something that should be done if there was time left from other obligations, the exergames worked best when included as part of the daily routine.
- A change of role: PD provided an approach for collaboration on an equal footing in a setting where the roles are often those of giving and receiving care.
- Organizational learning: Through the involvement of other stakeholders such as relatives, caregivers, managers at the care unit and enrolled nurses, rather than only those persons suffering from dementia, the special care unit as an organization was provided with an experience and opportunity for reflection on issues that are central for their work tasks, such as the development of service and content.
Conclusions
The results of these case studies indicate that the notions of games/competition, social interaction, physical activity and challenges are valuable ingredients for promoting well-being within dementia care. In our findings, the challenge of learning, the action and experience of physical movementand social interaction encapsulate what our participants describe as the motivating factors for success.
The use of exergames in these settings managed to bridge the gap between “being cared for” and being “active in life”. It managed to create the feelings of “being in control” and “handling the situation” for older people who often have to cope with losing their abilities. The exergames that we used managed to compensate for the participants’ physical weaknesses in fine motor skills that would have made it impossible for them to experience exhilaration on the golf course, in the bowling alley or in real-life water sports. The games provided an equal arena and fair competition among the participants. Furthermore, they set up an arena in which caregivers and gamers could meet and see each other from a different perspective, an action perspective where individuals played the new roles of gamers and perhaps even competitors, rather than the usual roles of patients and carers. In the second case study, a PD approach was not used. As a result, the organizations had difficulty establishing the exergames within their everyday activities. In these situations, the exergames were treated like an activity that was being offered. By contrast, in the settings where PD had been the main approach, the exergames became fully integrated and “theirs”.
These two cases are examples of how to discern a more integrated perspective on body movement and its value in enhancing cognitive, physical and social skills within dementia care. With this research, we hope to have made it clear that the forceful, vivid and focused movements we observed; movements that are usually hidden within dementia patients’ frail bodiescame out when the participants were motivated to be physically active through the enjoyment of exergaming activities. These results can hopefully be taken from research into design practice where similar design interventions can be implemented within dementia care and other fields.
Finally, we conclude with some comments and ideas for future research. It would be very interesting to investigate what a professional such as a recreation instructor could bring to settings such as dementia care units. The introduction of new resources such as exergames could support both the organizations and the older men and women who have to cope with different stages of dementia. Although there is no cure for dementia, the greater part of a patient’s day could still become more meaningful if more resources and different competences, or competences other than those already common within the caring professions were included in such settings. The next step following from our research would be to co-design new games or activities that make use of the tracking technologies included in exergame systems such as Nintendo or Kinect, while working in partnership with individuals suffering from dementia. The implementation of exergames in dementia care units is not to be seen as a quick fix. However, such implementations can be used as catalysts to reveal issues that need to be further addressed. The value of these game systems is enhanced by the eye-opening impact of the PD approach.
Acknowledgments
We are most grateful for the opportunity to learn and experience the power of playing together, designing together and succeeding and failing together with all the participants who made us feel so very welcome in their everyday settings. We thank the Assistive Technology for Elderly program for their financial support.
References
- Aarsland, D., Sardahaee, F. S., Anderssen, S., Ballard, C., & The Alzheimer’s Society Systematic Review Group. (2010). Is physical activity a potential preventive factor for vascular dementia? A systematic review. Aging & Mental Health, 14(4), 386-395.
- Adamovich, S. V., Merians, A. S., Boian, R., Lewis, J. A., Tremaine, M., Burdea, G. S., ... & Poizner, H. (2005). A virtual reality-based exercise system for hand rehabilitation post-stroke. Presence: Teleoperators and Virtual Environments, 14(2), 161-174.
- Alzheimer’s Australia. (2011). Consumer engagement in the aged care reform process. Retrieved November 13, 2015, from https://fightdementia.org.au/sites/default/files/20120410_ConsumerEngagementAgedCareReformProcess.REPORT.pdf
- Bamberger, J., & Schön, D. A. (1983). Learning as reflective conversation with materials: Notes from work in progress. Art Education, 36(2), 68-73.
- Bandura, A. (1994). Self-efficacy. In V. S. Ramachaudran (Ed.), Encyclopaedia of human behaviour (Vol.4, pp. 71-81). New York, NY: Academic Press.
- Bandura, A. (1997). Self-efficacy: The exercise of control. New York, NY: Freeman.
- Bannon, L. J., & Ehn, P. (2012). Design matters in participatory design. In J. Simonsen & T. Robertson (Eds.). Routledge handbook of participatory design (pp. 37-63). New York, NY: Routledge.
- Björgvinsson, E., Ehn, P., & Hillgren, P. A. (2010). Participatory design and democratizing innovation. In Proceedings of the 11th Biennial Participatory Design Conference (pp. 41-50). New York, NY: ACM.
- Björgvinsson, E., Ehn, P., & Hillgren, P. A. (2012). Agonistic participatory design: Working with marginalised social movements. CoDesign, 8(2-3), 127-144.
- Boulos, M. N., & Yang, S. P. (2013). Exergames for health and fitness: The roles of GPS and geosocial apps. International Journal of Health Geographics, 12, No. 18.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
- Brooker, D. (2007). Person-centred dementia care: Making services better. London, UK: Jessica Kingsley.
- Bødker, S., Ehn, P., Sjögren, D., & Sundblad, Y. (2000). Co-operative design–Perspectives on 20 years with “the Scandinavian IT design model”. Retrieved November 13, 2015, from http://cid.nada.kth.se/pdf/cid_104.pdf
- Bødker, S., & Sundblad, Y. (2008). Usability and interaction design–New challenges for the Scandinavian tradition. Behaviour & Information Technology, 27(4), 293-300.
- Cameirão, S. M., Bermúdez i Badia, S., Oller Duarte, E., & Verschure, FMJ. P. (2010). Neurorehabilitation using the virtual reality based rehabilitation gaming system: Methodology, design, psychometrics, usability and validation. Retrieved November 13, 2015, from http://www.jneuroengrehab.com/content/7/1/48
- Coen, R. F., O’Boyle, C. A., Coakley, D., & Lawlor, B. A. (2002). Individual quality of life factors distinguishing low-burden and high-burden caregivers of dementia patients. Dementia and Geriatric Cognitive Disorders, 13(3), 164-170.
- Dupuis, S. L., Gillies, J., Carson, J., Whyte, C., Genoe, R., Loiselle, L., & Sadler, L. (2012). Moving beyond patient and client approaches: Mobilizing “authentic partnerships” in dementia care, support and services. Dementia, 11(4), 427-452.
- Edberg, A. K., Bird, M., Richards, D. A., Woods, R., Keeley, P., & Davis-Quarrell, V. (2008). Strain in nursing care of people with dementia: Nurses’ experience in Australia, Sweden, and United Kingdom. Aging and Mental Health, 12(2), 236-243.
- Edvardsson, D., Winblad, B., & Sandman, P. O. (2008). Person-centred care of people with severe Alzheimer’s disease: Current status and ways forward. The Lancet Neurology, 7(4), 362-367.
- Ehn, P. (1992). Scandinavian design: On participation and skill. In P. S. Adler & T. A. Winograd (Eds.), Usability: Turning technologies into tools. (pp. 41-77). New York, NY: Oxford University Press.
- Ehn, P. (2008). Participation in design things. In Proceedings of the 10th Anniversary Conference on Participatory Design (pp. 92-101). Bloomington, IN: Indiana University.
- Emerson, R. M., Fretz, R. I., & Shaw, L. L. (2001). Participant observation and fieldnotes. In P. Atkinson, A. Coffey, S. Delamont, J. Lofland, & L. Lofland (Eds.), Handbook of ethnography (pp. 352-368). London, UK: SAGE.
- Fenney, A., & Lee, T. D. (2010). Exploring spared capacity in persons with dementia: What WiiTM can learn. Activities, Adaptation & Aging, 34(4), 303-313.
- Harmer, B. J., & Orrell, M. (2008). What is meaningful activity for people with dementia living in care homes? A comparison of the views of older people with dementia, staff and family carers. Aging and Mental Health, 12(5), 548-558.
- Hauer, K., Schwenk, M., Zieschang, T., Essig, M., Becker, C., & Oster, P. (2012). Physical training improves motor performance in people with dementia: A randomized controlled trial. Journal of the American Geriatrics Society, 60(1), 8-15.
- Hendriks, N., Truyen, F., & Duval, E. (2013). Designing with dementia: Guidelines for participatory design together with persons with dementia. In Proceedings of the 14th Conference on Human-Computer Interaction (pp. 649-666). Berlin, Germany: Springer.
- Holloway I., & Todres L. (2003). The status of method: Flexibility, consistency and coherence. In I. Holloway (Ed.), Qualitative research in health care (1st ed., pp. 90-102). Berkshire, UK: Open University Press.
- Häggström, E. (2005). Municipal care for old people: Experiences narrated by caregivers and relatives (Doctoral dissertation). University of Gävle, Stockholm, Sweden.
- Iivari J., & Lyytinen K. (1998). Research on information systems development in Scandinavia–Unity in plurality. Scandinavian Journal of Information Systems, 10(1 & 2), 135-185.
- Jolley, D., & Benbow, S. (2000). Stigma and Alzheimer’s disease: Causes, consequences and a constructive approach. International Journal of Clinical Practice, 54(2), 117-119.
- Kada, S., Nygaard, H. A., Mukesh, B. N., & Geitung, J. T. (2009). Staff attitudes towards institutionalised dementia residents. Journal of Clinical Nursing, 18(16), 2383-2392.
- Kahana, E., Kinney, J. M., Kercher, K., Kahana, B., Tinsley, V., & King, C. (1996). Predictors of attitudes toward three target groups of elderly persons. Journal of Aging and Health, 8(1), 27-53.
- Karp, A., Paillard-Borg, S., Wang, H-X., Silverstein, M., Winblad, B., & Fratiglioni, L. (2006). Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dementia and Geriatric Cognitive Disorders, 21(2), 65-73.
- Kemoun, G., Thibaud, M., Roumagne, N., Carette, P., Albinet, C., Toussaint, L., Paccalin, M., & Dugué, B. (2010). Effects of a physical training programme on cognitive function and walking efficiency in elderly persons with dementia. Dementia and Geriatric Cognitive Disorders, 29(2), 109-114.
- Klompstra, L. V., Jaarsma, T., & Strömberg, A. (2014). Exergaming in older adults: A scoping review and implementation potential for patients with heart failure. European Journal of Cardiovascular Nursing, 13(5), 388-398.
- Li, B., Maxwell, M., Leightley, D., Lindsay, A., Johnson, W., & Ruck, A. (2014). Development of exergame-based virtual trainer for physical therapy using Kinect. In B. Schouten, S. Fedtke, M. Schijven, M. Vosmeer, & A. Gekker (Eds.), Proceedings of the 4th Conference on Gaming and Playful Interaction in Healthcare—Games for Health (pp. 79-88). Wiesbaden, Germany: Springer.
- Lindwall, M., Rennemark, M., Halling, A., Berglund, J., & Hassmén, P. (2006). Depression and exercise in elderly men and women: Findings from the Swedish national study on aging and care. Journal of Aging and Physical Activity, 15(1), 41-55.
- McCallum, S., & Boletsis, C. (2013). Dementia games: A literature review of dementia-related serious games. In M. Ma, M. F. Oliveira, S. Petersen, & J. B. Hauge (Eds.), Serious games development and applications: Lecture notes in computer science (Vol. 8101, pp. 15-27). Berlin, Germany: Springer.
- Moelter, S., Glenn, M., Xie, S. X., Chittams, J., Arnold, S., & Clark, C. (2012). The dementia severity rating scale for dementia: Relationships with the CDR sum of boxes, clinical diagnosis and CSF biomarkers. Alzheimer’s & Dementia, 8(4), 132.
- Moyle, W., McAllister, M., Venturato, L., & Adams, T. (2007). Quality of life and dementia: The voice of the person with dementia. Dementia and Geriatric Cognitive Disorders, 6(2), 175-191.
- Paillard-Borg, S., Fratiglioni, L., Winblad, B., & Wang, H. X. (2009). Leisure activities in late life in relation to dementia risk: Principal component analysis. Dementia and Geriatric Cognitive Disorders, 28(2), 136-144.
- Piguet, O., Hornberger, M., Mioshi, E., & Hodges, J. R. (2011). Behavioural-variant frontotemporal dementia: Diagnosis, clinical staging, and management. The Lancet Neurology, 10(2), 162-172.
- Prince, M., Bryce, R., Albanese, E., Wimo, A., Ribeiro, W., & Ferri, C. P. (2013). The global prevalence of dementia: A systematic review and meta-analysis. Alzheimer’s & Dementia, 9(1), 63-75.
- Prince, M., Prina, M, & Guerchet, M. (2013). World Alzheimer Report 2013 - Journey of caring: An analysis of long-term care for dementia. Alzheimer’s Disease International. Retrieved November 13, 2015, from http://www.alz.co.uk/research/world-report
- Pykhtina, O., Balaam, M., Wood, O., Pattison, S., Kharrufa, A., & Oliver, P. (2012). Magic land: The design and evaluation of an interactive tabletop supporting therapeutic play with children. In Proceedings of the ACM Conference on Designing Interactive Systems (pp. 136-145). New York, NY: ACM.
- Rademaker, A., van der Linden, S., & Wiersinga, J. (2009). SilverFit, a virtual rehabilitation system. Gerontechnology, 8(2), 119.
- Robinson, L., Brittain, K., Lindsay, S., Jackson, D., & Olivier, P. (2009). Keeping in touch everyday (KITE) project: Developing assistive technologies with people with dementia and their carers to promote independence. International Psychogeriatrics, 21(3), 494-502.
- Rogers, Y., Sharp, H., Preece, J., & Tepper, M. (2007). Interaction design: Beyond human-computer interaction. New York, NY: Wiley.
- Scocco, P., Rapattoni, M., & Fantoni, G. (2006). Nursing home institutionalization: A source of eustress or distress for the elderly? International Journal of Geriatric Psychiatry, 21(3), 281-287.
- Seravalli, A. (2013). Prototyping for opening production: From designing for to designing in the making together. In Proceedings of the 10th European Academy of Design Conference. Gothenburg, Sweden: University of Gothenburg. Retrieved January 15, 2015, from http://medea.mah.se/2013/04/prototyping-for-opening-production-from-designing-for-to-designing-in-the-making-together/
- Sjögren, K., Lindkvist, M., Sandman, P. O., Zingmark, K., & Edvardsson, D. (2013). Person-centredness and its association with resident well-being in dementia care units. Journal of Advanced Nursing, 69(10), 2196-2205.
- Sterin, G. J. (2002). Essay on a word: A lived experience of Alzheimer’s disease. Dementia, 1(1), 7-10.
- Stessman, J., Hammerman-Rozenberg, R., Cohen, A., Ein-Mor, E., & Jacobs, JM. (2009). Physical activity, function and longevity among the very old. Archives of Internal Medicine, 169(16), 1476-1483.
- Swedish Council on Technology Assessment in Health Care. (2008). Dementia – Etiology and epidemiology. A systematic review. Retrieved January 10, 2015, from http://www.sbu.se/upload/Publikationer/Content1/1/Dementia_vol1.pdf
- Toth, N., Little, L. Read, J., Guo, Y., Fitton, D., & Horton, M. (2012). Teenagers talking about energy: Using narrative methods to inform design. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (pp. 2171-2176). New York, NY: ACM.
- Van Haitsma, K. S., Curyto, K., Abbott, K. M., Towsley, G. L., Spector, A., & Kleban, M. (2015). A randomized controlled trial for an individualized positive psychosocial intervention for the affective and behavioral symptoms of dementia in nursing home residents. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 70(1), 35-45.
- Whitehead, M. (2010). (Ed.). Physical literacy throughout the life-course. Oxford, UK: Routledge.
- Williams M. A., Soiza R. L., Jenkinson A. M., & Stewart A. (2010). Exercising with computers in later life (EXCELL) – Pilot and feasibility study of the acceptability of the Nintendo WiiFit in community-dwelling fallers. Retrieved November 13, 2015, from http://www.biomedcentral.com/1756-0500/3/238
